Minimally invasive neurosurgery
To reduce surgery-related injuries, the surgical incisions are kept as small as possible. “Keyhole surgery” entails obtaining sensitive healthy structures without losing the surgical overview. Benefits for patients include significantly reduced incision-related risks, a shorter and less stressful recovery period, and, if possible, complete healing through surgery. Cosmetic aspects also play an important role in planning the appropriate incision.
When creating an incision or working on soft tissues and the cranial bone, attention is paid to aesthetic compatibility, so that our patients may leave the hospital without having to shave their hair off and, if possible, without any disfiguring external changes.
Patient satisfaction is at the forefront of our efforts.
Neuroendoscopy
ENDOMIN Zurich – a Karl Storz Reference Centre

Endoscopes are special lens optics used for viewing and illuminating the surgical area. Better optical control is crucial when the minimally invasive incisions are reduced to the size of a keyhole.
The ENDOMIN Centre in Zurich provides special, internationally recognised expertise in the field of neuro-endoscopy.
The main advantages of an endoscope are improved light intensity in the surgical area, a clear presentation of deep structures, a vast depth of field, and the possibility to obtain a direct view of the averted edges in the operation area. Endoscopes can thus be used to improve the optical control during a micro-surgical procedure. Operations can be often performed exclusively using an endoscopic technique.
The ENDOMIN Centre in Zurich provides special, internationally recognised expertise in the field of neuro-endoscopy. As a reference centre of the Karl Storz Company, ENDOMIN College has organised numerous national and international training courses, meetings and conferences
Endoscopically assisted neurosurgery

There are various ways to employ endoscopes during a microsurgical brain operation. In endoscopically assisted neurosurgery, the surgeon primarily uses a microscope. The endoscope is implemented as an additional optical instrument in order to allow an even better orientation in the surgical area. Has the tumour been completely removed? Has the titanium clip been placed properly? Can the vascular sacculation be closed completely? We can provide reliable answers to these and other questions.
The use of camera, monitor and video systems – in particular, high-resolution “high definition” HD 3D technology – affords a brilliant endoscopic view. The optical systems can currently be combined with interactive information regarding operation planning or neuronavigation, as well as with the up-to-date ultrasound data, intra-operative computed tomography, magnetic resonance imaging, and angiography.
Optimal monitoring of surgical work achieved through the combination of different techniques in our ultra-modern operating theatres – this is our concept of minimally-invasive, endoscopically-assisted brain surgery.
Neuro-endoscopy in cavities of the brain

The first endoscopic procedures in neurosurgery were carried out in the cavities of the brain (i.e. cerebral ventricles) in order to treat cerebrospinal fluid circulation disorders. The dammed up and therefore expanded ventricular system provides an optimum scope of application. With the help of specially-developed endoscopes, the ventricular cavity can be reached through a borehole-like opening without the need for large-scale cranial trepanation. Blocked cerebrospinal fluid paths or cysts can be opened, and tumours can be removed in a minimally invasive manner through the narrow working channels.
A purely endoscopic surgery in the deep cerebrospinal fluid spaces via a slot-like opening in the skull – this is our concept of minimally invasive surgery of the cerebral ventricle!
Endoscopic transnasal skull base surgery

Tumours of the skull base and pituitary gland can often be reached through the nose via the transnasal access path. In most neurosurgical clinics, the skull base is reached by displacement of the nasal septum. Despite the expansion of the nasal cavity, the insight into the surgical area is quite limited. The surgeon may have difficulties assessing the laterally-situated tumour tissue. When operating without a direct view, the surgeon runs the risk of damaging important structures, such as the optic nerve or the carotid arteries.
However, when using the endoscope, the lateral structures become clearly visible. Each step can be safely monitored throughout the entire procedure. Direct visual control assures a complete removal of the tumour with the simultaneous protection of the healthy structures. An unpleasant tamponade of the nasal cavity is not necessary. Following the procedure, our patients are able to breathe freely through the nose.
In our centre, all transnasal endoscopic surgeries are performed in collaboration with the ORL Centre at the Hirslanden Clinic. This unique cooperation promises the greatest surgical success with minimal operational stress – this is our concept of minimally invasive endoscopic skull base surgery.
Endoscopy in Spinal Surgery

When it comes to herniated discs, the focus is on conservative physical treatment. Through the use of different techniques, the abdominal and back muscles are specifically trained, and pain is alleviated without the need for medication.
If the incident must be surgically treated because of refractory pain and/or paralysis, the lowest possible operational strain is crucial to shorten the post-operative recovery period. By using endoscopic and endoscope-assisted technique, the surgical access to the spinal column can be created carefully, thereby preserving the muscles. In purely endoscopic procedures, the herniated disc is removed through a small incision. Approx. 50% of herniated discs can be treated using dorsal or lateral incisions.
Larger and recurrent lumbar disc herniation, as well as degenerative spinal stenosis, are treated using endoscopically-assisted surgical techniques. The spine is reached atraumatically with the aid of a dilator system. This technique also reduces the incision-related injury – the incision is significantly smaller than it is in the case of “traditional” procedures. As a result of the low operational strain, our patients are mobilised as quickly as possible and are generally able to leave our clinic after a few days.
The purely endoscopic and endoscopically-assisted surgical techniques minimise surgery-related injury of the muscles and allow for a quick recovery following the surgery – this is our concept of minimally-invasive spinal surgery!
Neuronavigation and intraoperative imaging

In our surgery department, surgeons are supported by cutting-edge technology. The Hirslanden Clinic is home to the most modern operating theatres in Switzerland.
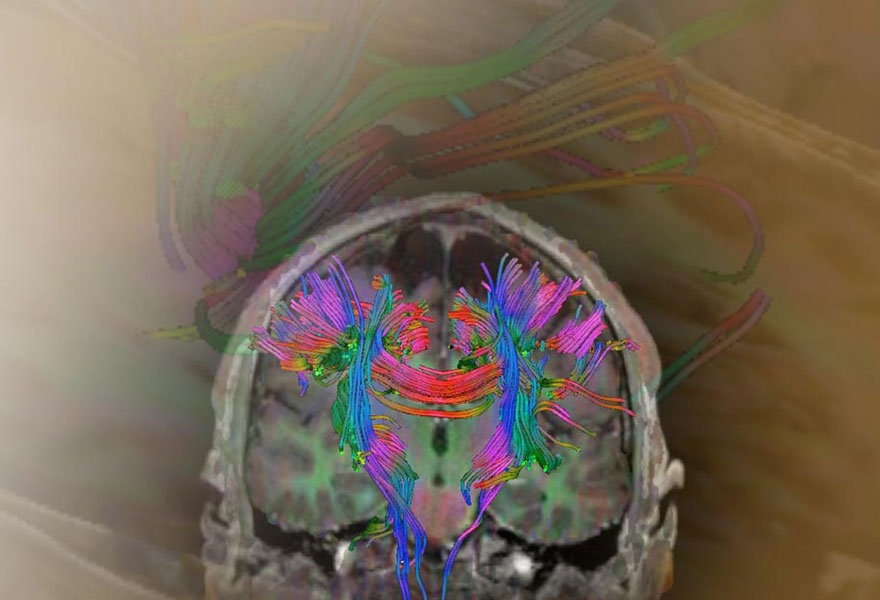
During minimally invasive surgery, we routinely use a navigation device. This is a computer-based method of image processing.
 It enables the transmission of image information into the operating room. The location and extent of a tumour can be projected onto the surface of the head and, after craniotomy, to the exposed areas of the brain. The imaging helps the surgeon to define the direction of incision and to reach the disease process in the gentlest manner. With neuronavigation, the tumour boundaries are optimally defined, as the computerised device facilitates anatomic and surgical orientation – even in critical situations.
It enables the transmission of image information into the operating room. The location and extent of a tumour can be projected onto the surface of the head and, after craniotomy, to the exposed areas of the brain. The imaging helps the surgeon to define the direction of incision and to reach the disease process in the gentlest manner. With neuronavigation, the tumour boundaries are optimally defined, as the computerised device facilitates anatomic and surgical orientation – even in critical situations.
During surgery, the effectiveness of the intervention is checked using intra-operative imaging. Residual tumour components can thus be located and removed safely. The Hirslanden Clinic has a unique infrastructure. Four neurosurgical operating rooms have been upgraded with the latest equipment and instruments.
The OR1 operating theatre was established with the support of Karl Storz – here, neuro-endoscopy is paramount. Microscope-based and endoscopic surgical techniques are optimally combined with electromagnetic or optical navigation. All devices in the room can be controlled from a central unit. The operational steps are also documented. The back lighting can be adjusted according to the preference of the surgeon, thereby creating a calming atmosphere for concentrated work.
In our BrainSUITE, we use intra-operative computed tomography (iCT), which is particularly advantageous in skull base surgery, as it allows for an aoptimal display of the bony and solid tumours of the skull base. When removing large tumours from the pituitary gland (pituitary adenoma) or operating on a benign tumour of the meninges (meningioma), iCT is the method of choice. Intra-operative MRI is used in the treatment of brain tumours. iMRI allows for a better display of the soft tissues of the brain.
 In this way, residual tumour mass can be displayed and removed, or surgical complications can be excluded. Although iMRI requires considerable technical effort, it is well worth it, since the complete resection of brain tumours demonstrably prolongs progression-free survival time.
In this way, residual tumour mass can be displayed and removed, or surgical complications can be excluded. Although iMRI requires considerable technical effort, it is well worth it, since the complete resection of brain tumours demonstrably prolongs progression-free survival time.
When caring for complex neurovascular lesions such as aneurysms and arteriovenous malformations, procedures are performed in our vascular hybrid operating room. By using intra-operative angiography, the result of an operation on the brain vessels can be monitored in a minimally invasive manner.
Fluorescence based surgery

Fast-growing and malignant tumours infiltrate the adjacent healthy tissue. The tumour margins are often difficult to define. The objective of minimally-invasive neurosurgery is a gentle yet radical resection – with the help of the 5-ALA fluorescence method. 5-aminolevulinic acid (Gliolan®) is dissolved in water and drunk 3-5 hours prior to surgery. The resulting protoporphyrins accumulate selectively in the tumour cells. During the operation, a blue light is emitted by the operating microscope. The tumour cells fluoresce in a salmon-red colour.
The combination of the 5-ALA resection technique, intra-operative MRI diagnosis, and endoscopic imaging allows for the maximum control of radical tumour resection and the preservation of cerebral functions.
The use of ICG fluorescence angiography (ICG: indocyanine green) affords a simple and risk-free way to monitor the results of a vascular operation during surgery (without X-rays) and to make immediate corrections if required. During surgery, the contrast agent is administered to the vein by an anaesthesiologist. By transmitting infra-red light through the microscope, the perfused vessels become visible. At the ENDOMIN Centre, this procedure is implemented during every aneurysm and angioma operation in order to ensure optimal results and so as to maximise the safety of the patient.
The combination of ICG technology and conventional intra-operative angiography in our hybrid operating room with the endoscopic imaging provides maximum surgical control in vascular neurosurgery.
Intra-operative monitoring
Additional verification and assurance of surgical work is achieved through intra-operative electrophysiological monitoring. By measuring brain waves, the functions of the brain centres can be checked during surgery, while vital structures are being protected.
In addition to monitoring the spontaneous electrical activity of nerve cells, the continuous dissipation of specific stimuli (evoked potentials) plays a major role. With the help of these evoked potentials, sensory and motor pathways as well as visual and auditory pathways can be monitored. Intra-operative monitoring thus yields two advances: it increases safety during surgery and allows us to remove tumours that were once considered inoperable.
If patients have suffered preoperative epileptic seizures and/or have displayed a pathological EEG (brain wave curve), intra-operative electrocardiography (ECOG) is performed during surgery. Potentially epileptic areas can be identified using electrode applied directly to the surface of the brain and removed if possible.
In special situations in which the tumour is in the immediate vicinity of the speech centre, memory centre, or motor centre, operations can be performed while the patient is awake. This is possible because the brain itself does not sense pain. Therefore, for operations in the awake state, only a local anaesthetic is required for the skin, the muscles, the bones of the skull and the dura mater. Patients undergoing such an operation mostly have positive experiences. They find it beneficial not to lose sight of the situation at any time. Before the operation, it is decided whether the patient is a suitable candidate for being operated on in the awake state. It is important to note that the patient may wish to discontinue the procedure in the awake state at any time. The operation can then be continued under a “proper” anaesthetic.
In skull base surgery and for tumours of the brain stem, the individual cranial nerves (e.g. the facial nerve, the ocular nerves and the glossopharyngeal nerve) and their nuclei of origin can be identified and thus protected.